Workforce Development

The goal of assuring a healthcare workforce able to support optimal adoption, use and advancement of health information and technology is complex. The range of competencies needed reflects the spectrum from healthcare delivery to pure IT, from data infrastructure to its collection and use, and from support of IT functions within healthcare delivery institutions to technology use by consumers.
The rapid change and advancement of IT broadly and specific to health IT itself, as well as rapid advances in both content and delivery approach of healthcare itself adds to the complexity. The impact of change on this complexity increases exponentially when we consider how advances in the two realms iterate and fuel each other. A final dimension of dynamic complexity comes from the social, economic and political environment in which we all operate.
In our contemplation of the evolving needs of the workforce to support health information and technology, we begin by examining the range of healthcare workforce competencies and capacities that must be supported. We then reflect on how current trends and the experience of the past year influence how we project our needs, and end by identifying opportunities and changes to our industry.
The Workforce Needed to Support Health Information and Technology
Over the past two decades, we have made remarkable progress in digitizing health information. Not only does this challenge the current healthcare delivery system, but it expands the user base to virtually the entire population. The health IT workforce must then support both an increasing range and complexity of technology and much greater breadth of its use and application.
The basic building blocks are a set of competencies that get combined into roles. The HIMSS job descriptions list identifies more than 50 discrete job titles, covering the range of clinical to highly technical roles, and by no means is this list exhaustive.
An effort by the Technology Informatics Guiding Education Reform (TIGER) international task force utilized expert survey input and global case studies to compile recommended core international informatics competencies reflective of many countries, scientific societies, and research projects. Together, the findings populated a recommendation framework to help measure, inform, educate and advance the development of a skilled healthcare workforce throughout the EU, U.S. and around the world.
The project resulted in a searchable database of more than 1,000 competencies representing five domains, five skill levels, and more than 250 roles
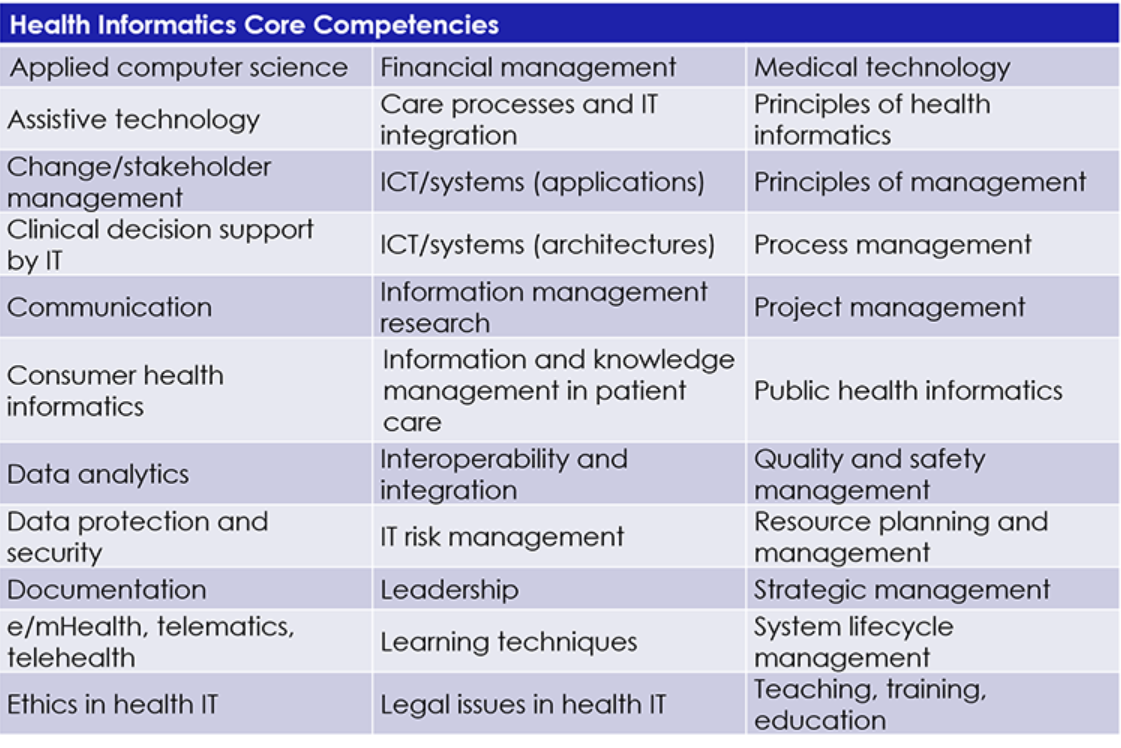
The competencies naturally bridge from technical to clinical, recognizing that health IT has the most impact when it can be practically used by care providers and consumers. To assure such practical use, communication and change management are key elements that underpin all successful efforts and must be part of any role or set of competencies.
Environmental Trends in Healthcare and Technology
A comprehensive discussion of trends in healthcare and IT are beyond the scope of this discussion, but it is worth recognizing a few high-impact developments for context.
As we look ahead, competencies identified—and perhaps some not yet recognized—will need to be prioritized to support shifts and innovations in alignment with these trends.
The following table begins to suggest the impact of significant healthcare trends on needs from the workforce.
|
Trend |
Implications for Workforce Needs |
|
Value based care/alternative care |
Integration of clinical and financial data collection, management, and analysis Support of new clinical tools |
|
Precision Medicine |
Advanced data analytics, access, implementation, and translation into clinical service delivery innovation |
|
Digital Health |
Wide range of skills and competencies ranging from technical support to workflow design and support and support of broader range of users in wider range of settings. |
|
Care anywhere |
Support of new and emerging technologies in settings and organizations beyond typical healthcare institutions |
|
Consumerism |
Increasing need for focus on support of consumers through extended and new roles |
|
Broader recognition of social determinants |
Need to extend access and support for health information technology to a broader range of service providers |
|
Integration of individual healthcare delivery and population/public health functions
|
Increased capacities to support interoperability, data analytics and reporting, application development and consumer engagement |
|
Advancement of data analytics/artificial intelligence
|
All aspects of data management and analytics, skills to advance AI, clinical leadership, interoperability, and workflow design |
|
Interoperability |
Data processes/standardization, clinical leadership and workflow integration, data governance, interface development and management, advancement of FHIR related capabilities. |
|
Cloud computing/ shift to software as a service |
Shift from internal physical IT infrastructure to service and contract management |
|
Threats to privacy and security |
Support for all aspects of privacy security assessment, planning, implementation, mitigation. |
|
Centralized models of clinical decision support |
Clinical informatics, interoperability, FHIR related support, clinical leadership |
|
Distributed research query infrastructure |
Data governance, data analytics, clinical informatics leadership and research design |
The Impact of Recent Experience
The past year has brought unprecedented challenges and change on a global level. The COVID-19 pandemic completely disrupted not only healthcare but every aspect of life. The need to rapidly support social distancing, and to integrate public health response into individualized patient care brought not only challenges, but impetus for rapid advancement in leveraging health IT enabled approaches. It also changed our appreciation of consumer needs and expectations.
Consumers now both expect and are expected to have more of their healthcare conducted remotely, rapidly emphasizing the needs identified above for skills to support digital health technology both technically and clinically, and to support consumers in their use of the technology. The delivery of care in atypical settings has also increased the base of vulnerability to privacy and security risk, exacerbated by unfortunate opportunism by attackers exploiting the pandemic. The pandemic also brought attention to the need for modernizing the technical and data infrastructure supporting public health, and the need to leverage interoperability to organize federated public health departments into a nationally coordinated system.
The past year also brought recognition of a second more insidious and far reaching public health threat, that of structural racism. The relationship of racism and inequities to healthcare and health outcomes must be addressed. Health IT can be a powerful tool to recognize and address health disparities. Technologies that improve access to care through digital health approaches, as well as data analytics and predictive modeling to identify disparities more effectively, their underlying causes and target interventions are examples. On the other hand, differential in technology access, education and digital literacy could exacerbate disparities if we do not deliberately address them.
Digital equity has emerged as a critical component to the success of health, education and economic wellbeing, amplified by the pandemic. A key component of digital equity is ensuring that public and private investments in digital connectivity and access are reaching all populations including rural, urban, disabled, racial/ethnic minorities and others. The high cost of computers previously viewed as the most significant barrier to benefitting from digital advancements is altered in an era of mobile devices that are more accessible. The digital divide has shifted to inequity between those who do and do not have bandwidth and those who may lack adequate digital literacy. Addressing these needs means assuring adequate workforce both in numbers and distribution and in terms of cultural relevance and competencies to make them effective.
The relevance to this discussion of healthcare workforce has several perspectives. Racial inequities exist in both employment rates, education and job development opportunities and salaries—these extend to health IT-related jobs. Furthermore, healthcare workforce shortages impact disadvantaged populations; this becomes more dramatic if we factor in the need for a workforce able to understand and relate to perspectives and needs of minority populations. Therefore, a two-pronged approach is needed: programs to create more health IT career opportunities for members of minority communities, and programs to increase the competencies of the broader workforce.
Of course, as the U.S. Office of the National Coordinator points out, application of health IT itself, including data analytics-based capabilities, has a role to play in identifying and addressing impact of health disparities. Failure to leverage these capacities could be considered an expression of structural racism.
Addressing health equity in our workforce involves more than opportunities for jobs or meeting individualized needs and preferences. We recognized the importance of change management and communication in the discussion of competencies. These have special meaning when we apply a health equity lens.
Finally, our notions of the workforce in general are altered in a post-COVID-19 world. Workers have had a taste of working in more flexible arrangements, free from old constraints of office-based schedules. Looking ahead, they have differing desires and expectations from their employers. Among these considerations it that more of our workforce desires to work remotely.
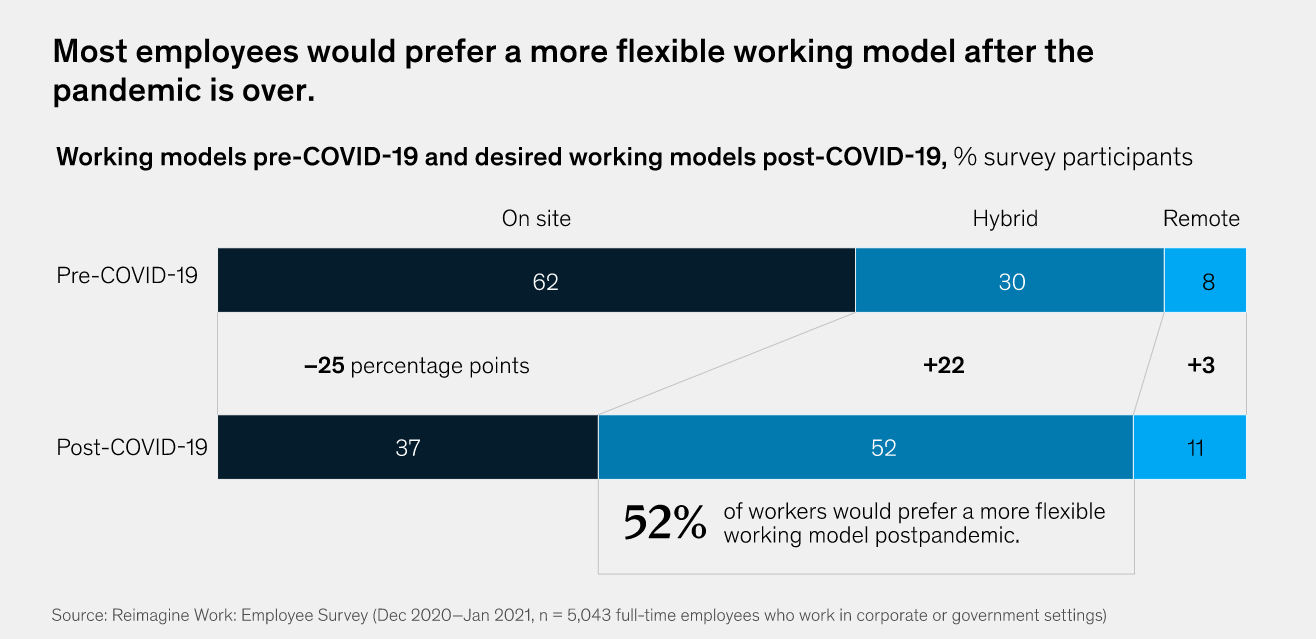
Source: McKinsey Reimagine Work Employee Survey
Time spent more closely with families has also altered notions of work-life balance and priorities.
As we transition to the next phases of recovery from COVID-19, in the U.S., the unprecedented federal investments allocated as part of the American Rescue Plan Act (ARPA) provide resources and opportunities to address deficiencies and gaps and to build future-oriented infrastructure and workforce. Overall ARPA contains $1.9 trillion in mandatory funding, programing and tax policies aimed at addressing the pandemic.
Among the provisions relevant to our discussion is that ARPA provides will provide $7.66 billion to carry out activities related to establishing, expanding and sustaining the healthcare workforce.
Looking Ahead
As we look ahead, we can anticipate the need to support increasing application of data and analytics integrated across more domains, more focus on supporting consumers directly, expansion to include a broader range of health-related and social services, continuing advancement and complexities of the range of digital health, ever-challenging privacy and security threats, and efforts to update and coordinate our public health infrastructure. At the same time, we must recognize the need to promote inclusion and equity in our workforce, and to recognize changing expectations around workplace flexibility and work-life balance.
Here then are some opportunities for our sector that are suggested by this discussion to build for the future.
- Continue to translate the comprehensive range of competencies identified into training and certification programs, job definitions, and development of career ladders
- Recognize changing notions of how we define and structure the workplace, including remote and flexible
- Develop strategies to improve diversity of the workforce by:
- Increasing inclusion of those from underserved and at-risk populations in the healthcare workforce through proactive training/education, recruitment, and job development initiatives
- Improving understanding and competencies of the entire workforce to address disparate needs and improve equity
- Advance a focus on the consumer by emphasizing and further defining roles and competencies that support consumer adoption and successful use of advancing health information and medical technologies
- Promote models that share human resources in areas of critical need or shortage across institutions, including a focus on smoothing deficits in populations in need and consideration of public utility models
- Support efforts to strengthen our public health infrastructure by engaging in innovative thinking and considering roles and new applications of competencies
- Leverage the global efforts around healthcare workforce competencies to identify approaches from other countries that might inform future models here in this country
- Provide vision and leadership in the utilization of ARPA funding to develop future oriented healthcare workforce and infrastructure
The views and opinions expressed in this content or by commenters are those of the author and do not necessarily reflect the official policy or position of HIMSS or its affiliates.
Related

Professional Development
On-Demand Webinars

Change Management
Articles

